A case of 18/F with metabolic acidosis and hypokalemia
http://akshithakasani81.blogspot.com/2021/09/general-medicine-case-discussions_21.html
Timeline of events and brief discussion of pathophysiology around it detailed below.
Slide 1-3, illustrate the timeline of events
She had symptoms of urinary urgency, frequency, stress incontinence , and was diagnosed as GUTB by biopsy
Slide 2: IV pyelography or IV urography which shows no enhancement on the right side suggesting a non functioning kidney on the right.
Bladder:contracted also called thimble bladder ,
TB frequently involves the GUT(genito urinary tract)-2nd most extra pulmonary involvement
Kidney>bladder>fallopian tube>scrotum
ATT regimen is same as for newly detected sputum positive -6months(2+4)
Slide 4: 3 ABG's at three different scenarios in her
Dec'20: 1 month post surgery followup
April:1st presentation with quadriparesis thought to be GB , corrected with potassium replacement
Sep'21:last admission with vomitings ,pre renal Aki
How to read this abg?
Step 1: there is acidosis as the pH is less than 7.35
Step 2: is there compensation ? For the obvious reason that pH has not normalised there is no adequate compensation
Step 3:acidosis : is either due to respiratory or metabolic
As pco2 is less than 32 it is metabolic
Step 4: metabolic acidosis- is it a simple disorder or mixed
In case of mixed: is this respiratory /metabolic
Respiratory compensation can be checked via winter's formula
Expected pco2:(1.5*hco3)+8+/-2
Abg1:21.8+/-2
Abg 2: 15.5+/- 2
Abg 3: 11.9+/-2
Pco2 is within normal expected range suggesting that there is no respiratory mixed disorder
Why did I suspect a respiratory disorder?
Because of possibility of pulmonary Koch's causing respiratory alkalosis...
Step 5: metabolic mixed disorders
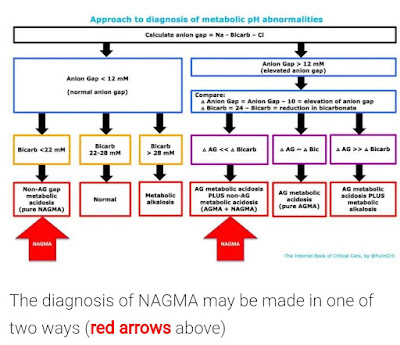
The evaluation is in slide 5:
https://emcrit.org/ibcc/nagma/
The anion gap has to be calculated
A.G: Na-(Cl+hco3-)
Going by the history :the patient is expected to have normal anion gap acidosis post ureterosigmoidostomy but instead she has high anion gap
(Pathophysiology illustrated later)
Step 6:
Check for Delta gap
∆A.G/∆Hco3
(∆A.G: A.G-10
∆hco3: 24-hco3)
The significance of this is less than 1 :indicates presence of both nagma+hagma
1-2:pure hagma
>2: hagma+metabolic alkalosis
So going by this flowchart
The delta gap was
Abg1: 0.8(hagma+nagma)
Abg 2: 0.8(hagma+nagma)
Abg 3: 1(hagma)
The cause for nagma :
Slide 7:
https://derangedphysiology.com/cicm-primary-exam/required-reading/acid-base-physiology/acid-base-disturbances/Chapter%20505/ureteric-diversion-cause-normal-anion-gap-acidosis
Urine delivered to the bowel is rich in ammonium. This ammonium substitutes for potassium in a co-transporter. Action of the co-transporter facilitates the resorption of 2 chloride ions for every resorbed ammonium and sodium ion. This results in a net gain of chloride for the body fluids, decreasing the strong ion difference. In parallel, potassium is left behind in the urine.
Possible causes for hagma could be
? Starvation ketoacidosis : as the patient was thin built with decreased intake of food due to side effects of bicarbonate therapy
?renal failure : due to pre renal Aki over single functioning kidney.
Lactic acidosis type A: due to hypoperfersuion, as she had hypotension on the last presentation
Further reading on Delta gap and significance:
https://derangedphysiology.com/cicm-primary-exam/required-reading/acid-base-physiology/Chapter%20705/delta-gap-and-delta-ratio
Delta gap is essentially a tool to determine whether or not there is also a normal anion gap metabolic acidosis present. The normal value for delta gap is zero, and it should remain zero as anion gap and bicarbonate change together (mole for mole, in opposite directions). If the bicarbonate is changing significantly less than the anion gap, the delta gap will become more and more positive, reflecting the fact that an alkalosis is present. If the change in bicarbonate is significantly greater than the change in anion gap, there is clearly some acidosis present which is unrelated to the anion gap rise, and the delta gap will be very negative.
Donald.E.Wesson:guide to metabolic acidosis.
Management:
Acute management :replacing potassium,bicarbonate
Rectal drain:to reduce the amount of time the urine is in contact with intestinal mucosa.
For this patient what else could have been done:
https://www.spandidos-publications.com/10.3892/etm.2019.8111
This procedure is basically undoing the mainzII technique and allowing lesser contact of urine with bowel segment.
The results from the therapeutic trial for 6 patients were promising
The follow-up of patients post procedure 1 week,3 months,3 years
Which showed improvement in bicarbonate, pH, base excess,potassium.









Comments
Post a Comment